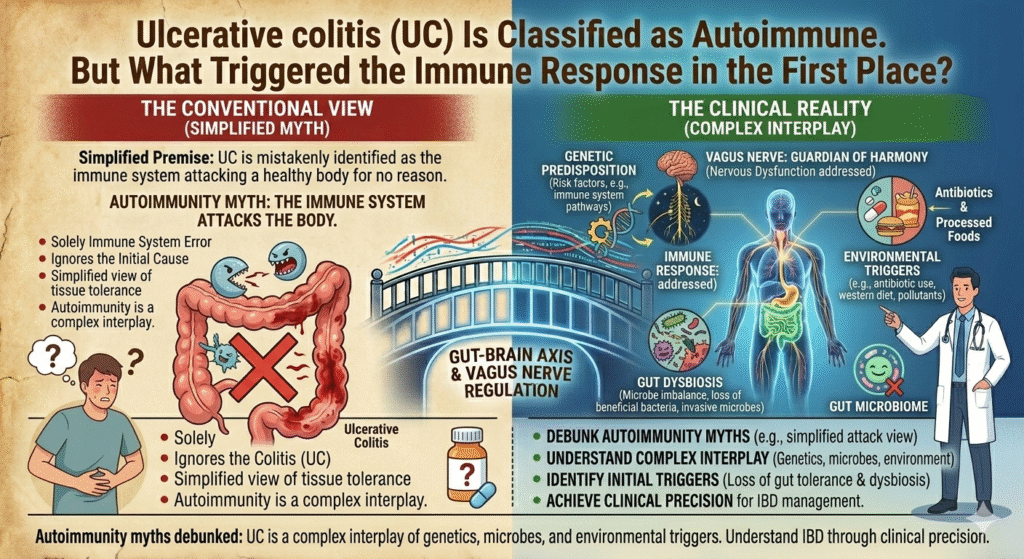
Myth: Ulcerative colitis (UC) is solely an autoimmune disease, mysteriously attacking the body. The truth is less enigma, more physiology. UC, a critical form of IBD, is most often depicted as the result of the immune system running amok, but this portrayal is woefully simplistic. Instead, the ailment emerges from a precise confluence of genetic susceptibility, gut microbiome disturbances, and environmental triggers. These factors ignite an immune response that is too intentional to be arbitrary.
Environmental Triggers: The Layer Others Overlook
While genetics constructs the stage for ulcerative colitis, environmental exposures pull the trigger. Long-term use of antacids and PPIs alters stomach acidity, disturbing microbial balance and allowing pathogenic bacteria to propagate. This isn’t a matter of chance but a direct attack on mucosal barriers that the immune system can’t ignore. A disrupted gut microbiome sends continuous maladaptive signals through the vagus nerve, distorting the gut-brain axis and promoting inflammation.
Certain phospholipases, like Phospholipase A2, play an integral role by releasing arachidonic acid, giving birth to pro-inflammatory eicosanoids. These enzymes don’t act independently; they’re activated under specific conditions, such as the chronic imbalance of gut microbiota. Viewing ulcerative colitis purely as an autoimmune escapade misses the cascade initiated by these external agents.
This frame of external influences and enzymatic responses builds a narrative that is far more grounded in clinical truth than the ghostly specter of rogue genes and immune cells.
The Vagus Nerve and Nervous System Dysregulation
To comprehend ulcerative colitis, one must consider more than the visceral reaction. This autoimmune condition is intimately tied to the enteric nervous system via the vagus nerve. The vagus nerve isn’t merely a pipeline; it’s an arbiter of autonomic regulation. Its bi-directional signals between the gut and the brain elaborate the body’s inflammatory responses. Arbitrators like the dorsal vagal complex component of Polyvagal Theory explain physiological shutdown and dysregulation when chronic inflammation is present.
When the inflammatory cycle persists, vagal tone diminishes. This myriad of signals from an inflamed gut prevents accurate autonomic regulation, perpetuating a state of ‘freeze’ in polyvagal terms. Unresolved, this can culminate in altered emotional patterns impacting the hypothalamic-pituitary-adrenal (HPA) axis. This cascade explains why ulcerative colitis feels like more than just a gut issue it’s an entire systemic affair.
Understanding the role of the vagus nerve shifts ulcerative colitis from a mere autoimmune misadventure to an orchestrated physiological process.
A New Perspective on Autoimmunity in UC
Common medical narratives oversimplify the immune response in UC as self-destructive chaos. In reality, the immune system naturally reacts to complex triggers inherent in genetically susceptible individuals. Immunologic checkpoints like T regulatory cells are derailed by exacerbated antigenic load combined with previous vagal disturbances. The enzymatic culprits in metabolizing these antigens, including cytochrome P450 isoforms, might not function optimally due to ongoing dysregulation.
Excessive PPIs and antacids distort these biochemical pathways, accumulating metabolites that otherwise should signal immune clarity. This results in a misdirected immune assault mirrored in UC. The approach should never be only symptom suppression but the deciphering of these physiological abnormalities that wring out the body’s immune faculty.
Naming these mechanisms reframes UC as not just an overactive immune response, but a consequence of distinct biochemical terrains gone rogue.
Understanding ulcerative colitis through this precision lens, it becomes clear autoimmunity isn’t a medical enigma. It’s a clinical reality bound by physiological truths.
Meta Description:
Autoimmunity myths debunked: UC is a complex interplay of genetics, microbes, and environmental triggers. Understand IBD through clinical precision.